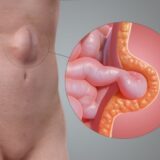
Ventral hernias are typically diagnosed by checking the abdomen for a noticeable bulge. Some physicians may conduct CT scans, ultrasound, blood tests, or urinalysis in addition to the physical examination. A ventral hernia’s symptoms are determined by its location in the abdomen and can include sharp pain that may be present during physical activity, vomiting (in the case of incisional hernias), and constipation.